Tear of anterior cruciate ligament(ACL)


Mitsutoshi Hayashi
Mitsutoshi Hayashi
Doctor of Medicine, specialist in the Japanese Society of Rehabilitation Medicine, specialist in the Japanese Society of Orthopaedic Surgery, specialist in the Japanese Society of Rheumatology, staff to strengthen JOC, and sports physician certified by the Japan Sports Association
Tear of anterior cruciate ligament(ACL)
Anterior cruciate ligament rupture occurs spontaneously even in non-contact sports.
Disease Overview
Anterior cruciate ligament (ACL) rupture, the most severe injury of sports injury of the knee, can affect athletic activities. It happens commonly in contact sports, and treatment is prolonged. Please be careful that halfway treatment induces rather prolonged treatment terms and after the treatment it does not necessarily result in a better prognosis.
Cause and mechanism of onset
Functional anatomy
The ACL runs in two bundles from the lateral femur to the medial tibia within the knee joint. The ACL functions as a stopper for sports activities to not break the knee when the person takes motion such as jump, landing, dash, stop, cut, or twist. ACL stabilizes the knee joint when anterior mobility of the lower leg, internal rotation of the lower leg (torsion), and pivoting movement are conducted.
Cause of the injury
It is more likely to occur in contact sports that tackle to the knee. The injury sometimes occurs when the athlete jumps and lands such as in a non-contact sport like basketball or volleyball, when a pivot is forced, or when the one slips.
Sports likely to cause the injury and gender differences
These sports include American football, rugby (e.g., during external and posterior tackling), skiing, snowboarding (where the board is fixed and the knee is forced to rotate), judo, basketball (where people are hit when the jump is landed), and volleyball (self-harm due to slip). The site of ligament injury may actually be changed by a tackle above the knee, below the knee, or if the foot has been secured. In volleyball and basketball women much suffer the injury.
Symptoms
Acute phase: Pain that starts suddenly after an injury, impaired knee movement, swollen joints or hematomas, and knee collapse (the knee does not work and falls when landing) may appear. If pain persists still after 2 to 3 weeks, meniscus injury is suspected.
Diagnosis
Testing
In the acute phase, joint hematomas and flail joint are caused. Manual tests are positive for anterior pull-out, Rackman test (flexion position of the knee about 20 degrees), and the Pivot Shift test (N-test). MRI is the most helpful procedure. It can detect not only ACL but also other ligament injuries, meniscus injuries, hematomas, and bone injuries. Mobility of the knee joint can be checked with a telos or other instrument.
An X-ray helps check for fractures, but does not show ligaments. Arthroscopy (endoscopy) is the most useful and reliable method of diagnosis, but it is invasive as a surgical procedure, with a skin incision and anesthesia. The ACL is rarely injured alone and is often combined with medial collateral ligament injury or meniscus injury.
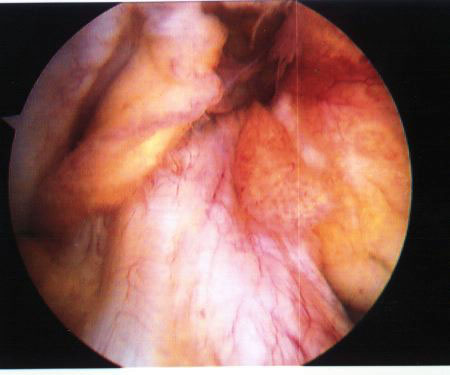
Photo: Arthroscopic photograph of an ACL mild injury. The ligaments are relaxed, but their morphology is preserved.
Treatment and rehabilitation
Treatment
In principle, ACL reconstructive surgery is necessary when adolescent athletes maintain a high level of sports activity. Currently, surgery is usually performed by implanting the own tendon (such as a semitendinosus tendon or a patellar tendon with a bone). Because the ACL is present in the knee joint, it is a negative factor that when collateral blood flow from other parts of the body is poor and ruptured, direct suturing does not restore blood flow, and the tendon is difficult to agglutinate. Consequently, ligament reconstruction with tendon grafting is the mainstream of surgery. Reconstruction with prosthetic ligament, which is previously prevalent, is now less common.
Immobilization with a cast or brace for a long time from the initial stage is a way of the conservative treatments. However, it is important to understand that, with conservative treatment, it is difficult to restore the function of the ACL itself due to loosening of the tendon, and that the purpose of treatment is to restore ADL (activities of daily living), maintain and strengthen muscle strength around the knee, and maintain competitive performance. Early in the injury, it is recommended that immobilizing the joints or the icing measurements.
Medical rehabilitation
Check points during training are as follows:
(1) whether the knees do not collapse while walking in daily life,
(2) Availability of running,
(3) Availability of climbing and descending on stairs,
(4) Availability of jumping with both legs,
(5) Availability of dashing, and
(6) Availability of jumping with a leg.
If knee collapse does not recur during exercise or skiing after treatment or if it occurs, the knee should be re-examined for surgical treatment. There is a risk of meniscus injury or articular cartilage injury.
Rehabilitation menu
(1) Two to three weeks after surgery (if a patient has conservative treatment, after the injury), one begins full weight-bearing walking with an orthosis. Start with less weight-bearing, underwater walking, flutter kick, crawl, flat swimming, and aerobics.
(2) Once no knee pain or swelling has been confirmed after doing the exercise listed above, gradually stressing exercises is recommended such as running, stepping jumps, calf raise, leg curls, and uncoordinated leg movements with no load (hip joint flexion, knee flexion, ankle dorsiflexion, extension, plantar flexion).
(3) Finally, a half squat, balance board, sliding, calf raise. and trampoline are used to re-educate the sense of balance around the knee.
(4) If it is confirmed that there is no problem from the exercises above, please perform more active sports gradually. However, each performance requires a monthly training period.
Prognosis
The period to return to sports varies but it is said to take at least 6 months, but it actually takes up to 8 months and generally more than 1 year. In many cases, joint loosening persists with halfway treatment and rehabilitation.

Hitoshi Takahashi
Hitoshi Takahashi
Associate Professor, the Department of Regional Medicine, Teikyo Heisei University
A certified athletic trainer from the Japan Sport Association, a practitioner of acupuncture and a massage practitioner
Rupture of anterior cruciate ligament of knee
Prevention
Introduction
Anterior cruciate ligament injuries, along with medial collateral ligament and meniscal injuries, are typical sports injuries of the knee joint. The patient’s age range varies from high school to middle-aged and senior high school students, and activity levels range from leisure sports to professional levels.
Treatment of anterior cruciate ligament injuries may be conservative or surgical (ligament reconstruction). In recent years, arthroscopic reconstruction of the ligaments is common.
On-site evaluation and first aid
There are two types of injury. One is contact type that is caused by tackles and other movements and the other one is non-contact type that is caused by twisting the knee during movement. The knee joint often swells during injury which makes knee loading difficult. In the first-aid treatment, it is recommended that the knee joint is fixed with a splint or the like, and the entire knee joint (front side, posterior side, and lateral side) is iced. Afterwards, see medical specialists as soon as possible.
Reconditioning
As ACL is often occur during sports activities, to return to sports, medical rehabilitation and athletic rehabilitation for the acquisition of sporting ability needed for sports activities are required.
This time, I explain the basic actions of the steps performed in athletic rehabilitation about three months after surgery. The basic action of the step is not simply to accustom movement. It is necessary to prevent re-injury while performing the movement and to becoming aware of the nature of the movement (to create the movement) that does not stress the anterior cruciate ligament. During the movement, it is important that the knee joint should not be rolled outward, and not tilting the center of gravity backward.
With the toes and knees in the same orientation
Do not attempt to turn the knees inward with the toes opening outward while moving, because this induces knee valgus and stresses the anterior cruciate ligament. Therefore, the toes and knees should always be in the same orientation during movement. Particular attention should be given to changing in direction or turning off a side step.
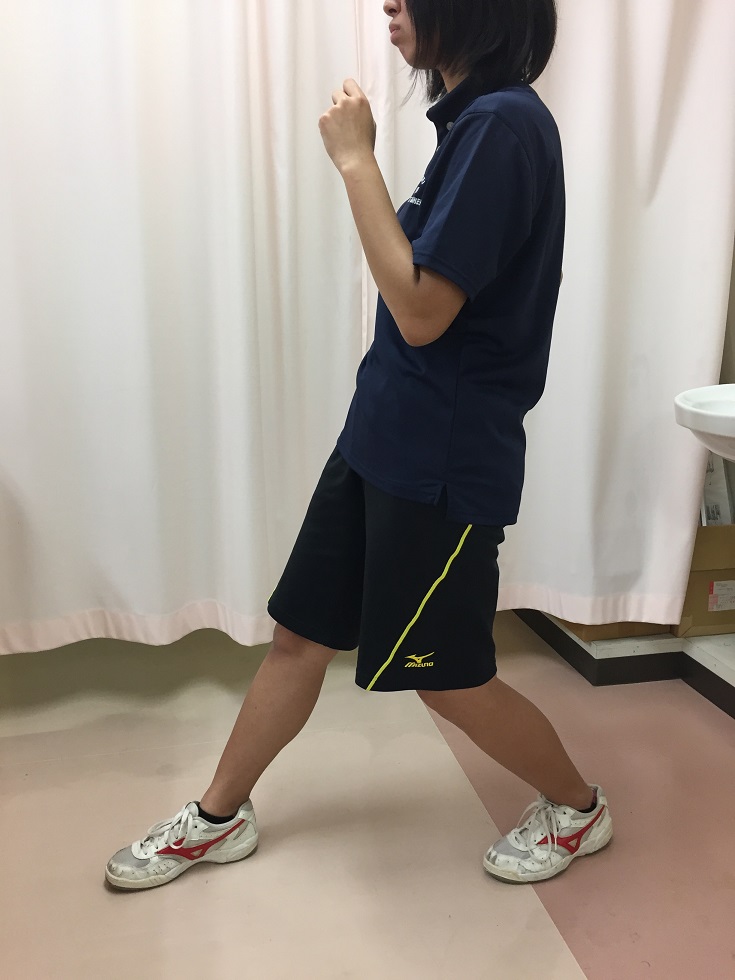
Harkee
Introduce the harkee (stepping the leg quickly on the spot). Doing the harkee, be aware that the stance between the left and right foot is not too wide. Keep the hip joint and knee in a lower position so that the center of gravity does not tilt backward.

Keep the heel up (weight on the ball of the foot) and flex the hip joint and knee joints to maintain a lower position during the movement.

Example of a bad posture in which the upper body goes up.
Stopping movement training
Stopping movement in small steps with the harkee. Do not stop the backward center of gravity, like landing suddenly as shown in the first photo. Stopping movements needs keep the person in a lower position and stops the action in small steps.

Stopping movements, landing in one big step, tend to result in a backward center of gravity.

Please keep the knee joint and hip joint in a lower position when stopping movement
Side step
Please move toward side from harkee. As soon as the foot is stepped in the moving direction, the opposite foot should be pulled. The toes and knees are always facing front side. Please do not take steps that pull the leg or widen too much as they may cause knee valgus.

Backward step
Please move backward as the foot moves backward (in the direction of progression) while keeping the lower position. Upper position caused center of gravity backward.

Maintain a lower posture and move the foot posteriorly.
A higher posture and a backward center of gravity.
Combination of movement
For example, combine the movements as follows: harkee, stopping steps, side steps, backward steps. Please be aware to keep posture when you move to the next action.
