Groin pain syndrome


Mitsutoshi Hayashi
Mitsutoshi Hayashi
Doctor of Medicine, specialist in the Japanese Society of Rehabilitation Medicine, specialist in the Japanese Society of Orthopaedic Surgery, specialist in the Japanese Society of Rheumatology, staff to strengthen JOC, and sports physician certified by the Japan Sports Association
Doctor's Editon
Disease Overview
These are described as inguinal pain syndromes (Groin pain syndrome) because many types of groin area pain occur in football and other sports from various causes, making it difficult to identify the true cause.
Differential diagnoses include symphysis pubis inflammation, enthesitis of the adducent muscles of the femur, rectus femoris myositis, rectus abdominis enthesitis, iliopsoas myositis, and inguinal hernias.
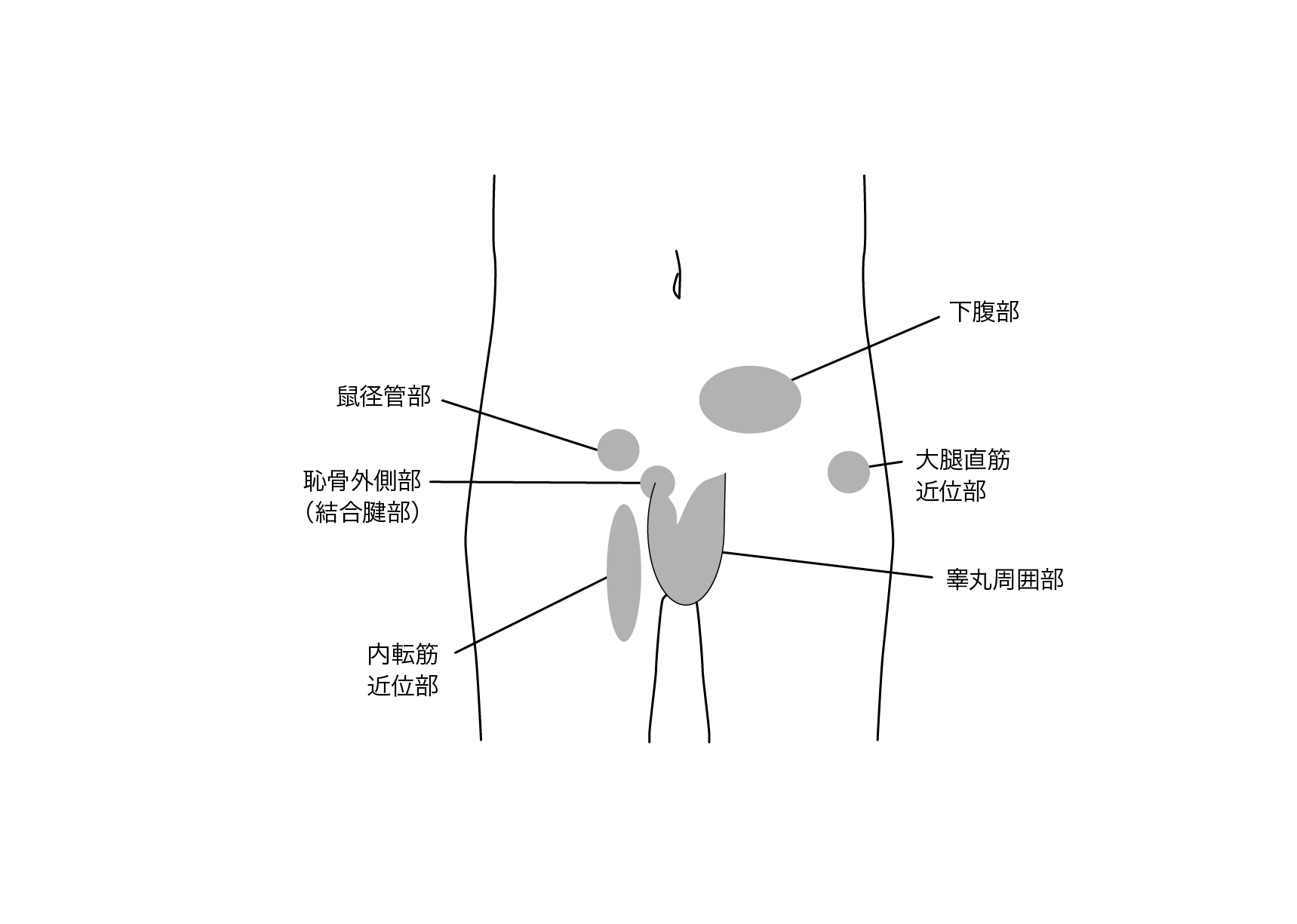
Figure: Area of pain around the groin (Reference 1).
Cause and mechanism of onset
Cause of the injury
Muscle weakness, decreased flexibility, and contracture may be caused by injury or overuse in sports of the leg. And it seems to lead to pain around the inguinal region.
Repeated exercises, such as kicking and running, can inflame and hurt the groin, hip joint, and pelvis through mechanical stress. It also occurs when a person has a direct blow to the hip joint area, such as a tackle.
Symptoms
It is characterized by tenderness, motor pain, and sometimes pain radiating to the groin, medial thigh (adducent muscles insertion), or lower abdomen. Chronic pain always affects the groin. It is particularly likely to be triggered by activities that extend, raise, and abduct the lower extremities, resulting in limited range of motion and weakness muscles of the hip joint.
Common sports
Soccer is the most common type of sport, and it is most common among male athletes around the age of 20, including, track and field, rugby, hockey, and weight lifting.
Diagnosis
A definite diagnosis is difficult to make for pain around the groin.
Differential (similar) diagnosis
Symphysis pubis inflammation is inflammation caused by exercise stress on the cartilaginous disks that unite the pubic bones on both sides of the body. It is often a disorder caused by sports.
Typically, symphysis pubis inflammation causes bone lysis at the pubic junctions of the gracilis and adducent muscles, differences in the height of the right and left pubic bones, and deformities of the symphysis. It can also be seen on CT. However, changes to the bones are relatively uncommon.
Pubic stress fractures occur mainly in basketball and tennis, especially involving pain in the groin area.
These include buttock pain due to hamstring injury, iliotibial band syndrome with lateral thigh pain, and gluteal myositis.
Treatment and rehabilitation
Treatment
Conservative therapy is the first choice in patients with acute disease or within the first six months of onset. People with severe pain may need to stop sports for about 2 weeks. Local bed rest, ice, sometimes heat therapy (hot packs), anti-inflammatory analgesics, and topical injections of steroid hormones (avoided for multiple uses) may be used, but exercise therapy may be effective in the long term.
Early rehabilitation begins with hip joint range-of-motion abduction exercises, muscle strengthening, and adducent muscle stretching, followed by underwater walking, exercise bike followed by jogging, and ball-kick exercises in 2 months. As the pain disappears, please do not judge to return to sports because it may lead to recurrence. Chronic disease requires long-term (more than 2 to 3 months) cessation of sports, so caution is needed.
Surgery
Surgical treatment may be considered if the pain persists for a long time despite conservative treatment. However, conservative treatment has been successful, and rehabilitation is performed aggressively.
Reference: 1) Niga Sadao: Groin pain syndrome

Hitoshi Takahashi
Hitoshi Takahashi
Associate Professor, the Department of Regional Medicine, Teikyo Heisei University
A certified athletic trainer from the Japan Sport Association, a practitioner of acupuncture and a massage practitioner
Trainer's edition
Prevention
Preventive measures include ensuring muscle flexibility around the hip joint and strengthening the trunk and hip joint muscles. Football players also improve their sports activities, such as learning kicking movements in which the lower and upper limbs are connected.
On-site evaluation and first aid
People who complain of hip joint pain at a sports site should first seek medical attention for structural problems (such as inguinal hernias or stress fractures). If there is no organic problem, it can be managed as a functional problem (peri-inguinal pain syndrome). If the pain is severe, the person should stop sports and wear ice.
Reconditioning
Stretching
Players who are considered to have peri-inguinal pain syndromes characteristically have reduced flexibility of the muscles surrounding the hip joint. Of particular importance is maintaining hip joint adductor flexibility. This section describes the stretching of the adducent muscles surrounding the hip joint, the extensor muscles (gluteus maximus and hamstrings), and the flexor muscles (iliopsoas and rectus femoris).
Stretching is done statically for 10 to 20 seconds.
Adducent muscles
1 (cog split)
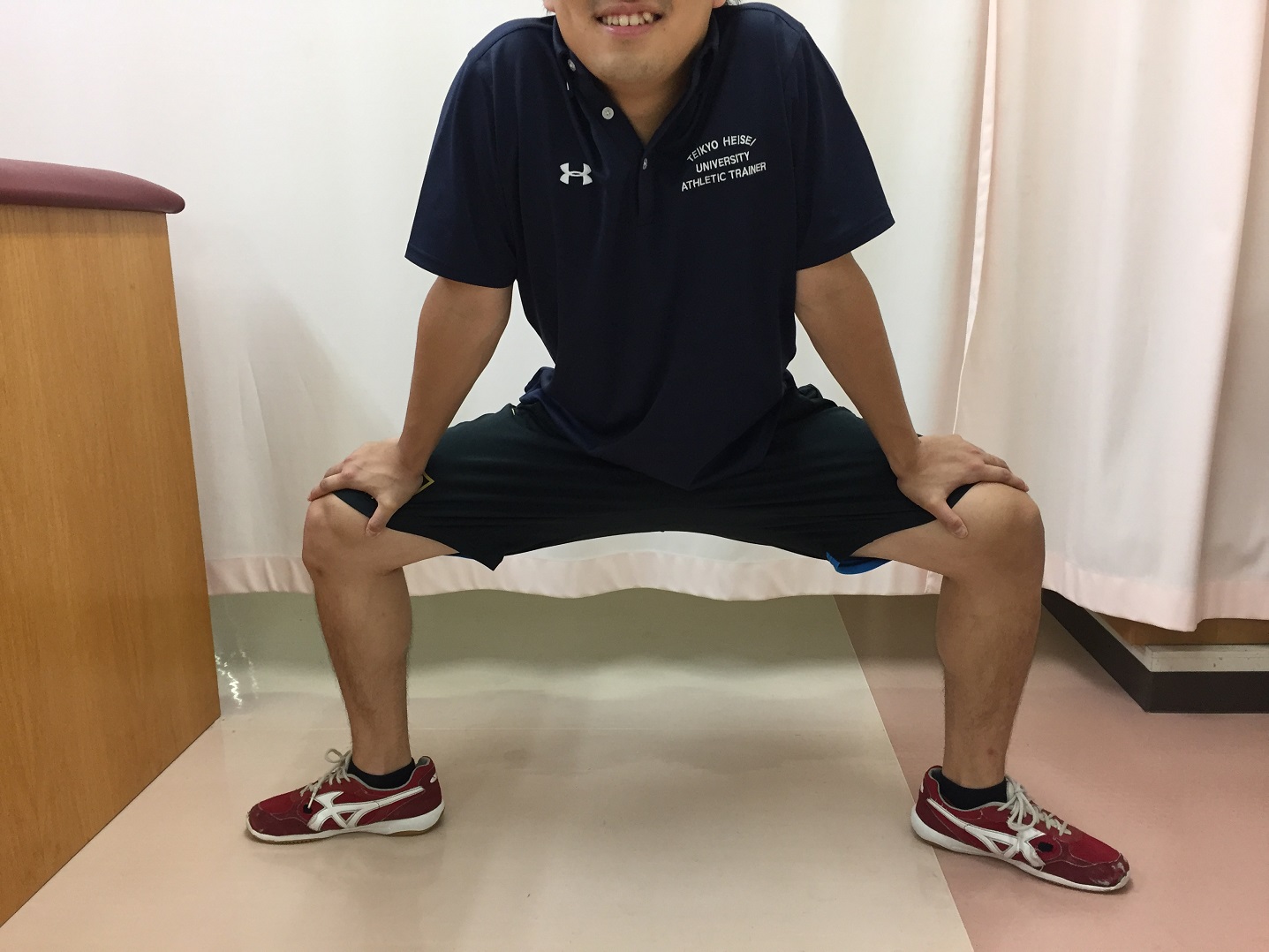
Place the toes and knees in the same direction. Drop the lower back until stretching is felt in the medial thigh.

Push the shoulder forward and push the inside of the knee
2: (extensor leg)
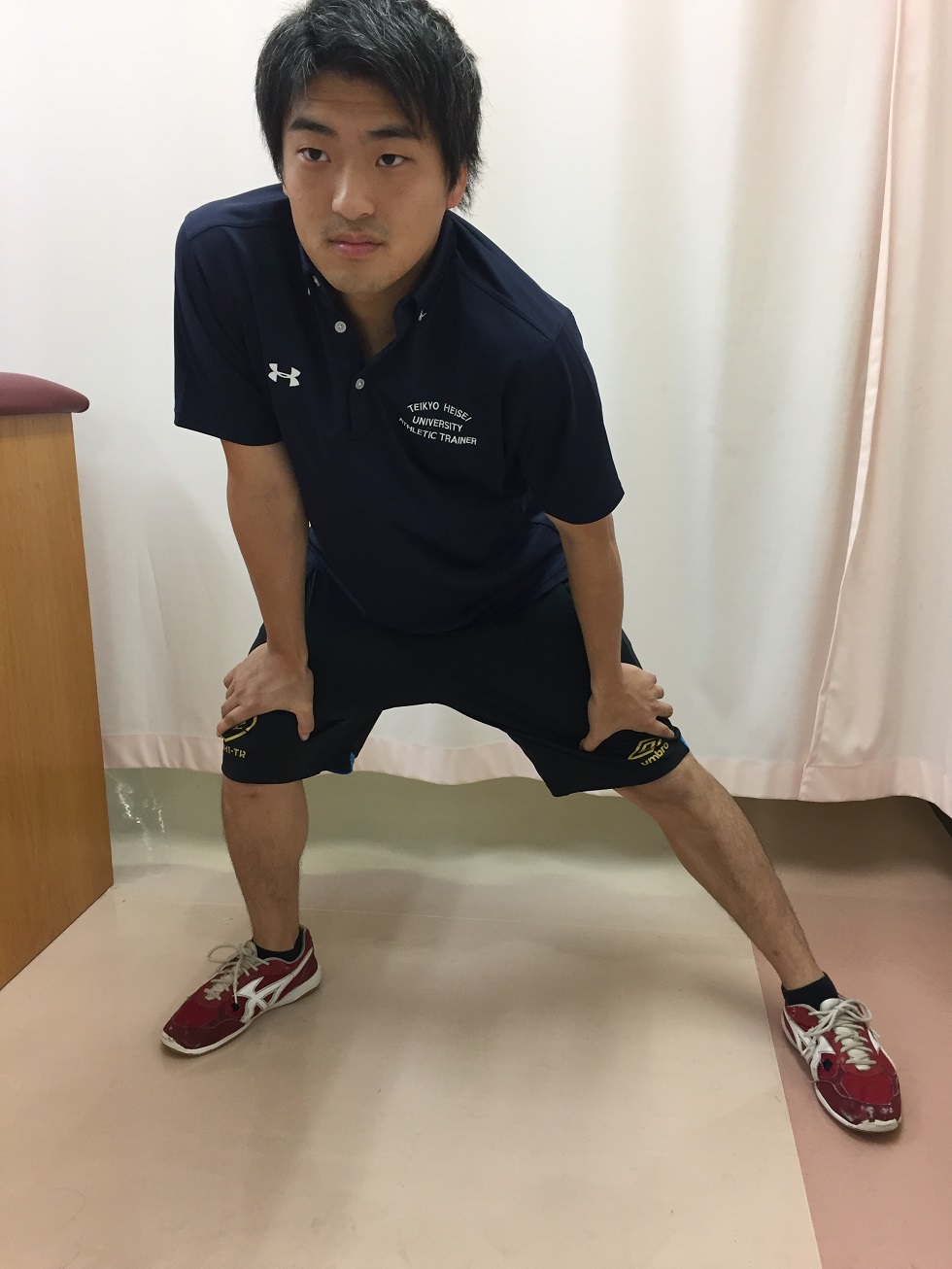
Push gently over the knee and thigh of the extended foot.
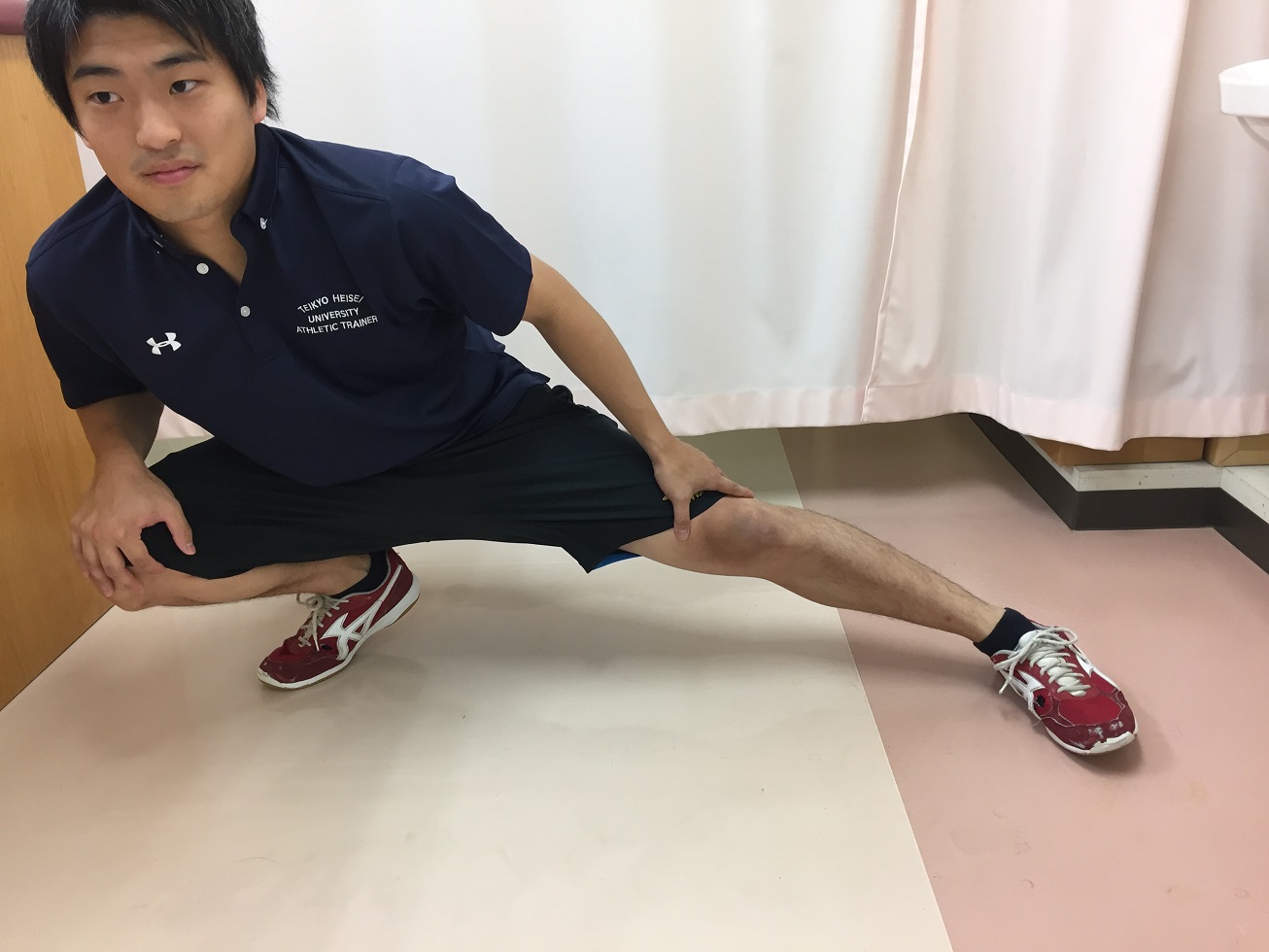
Lower posture (Photo 4)
3
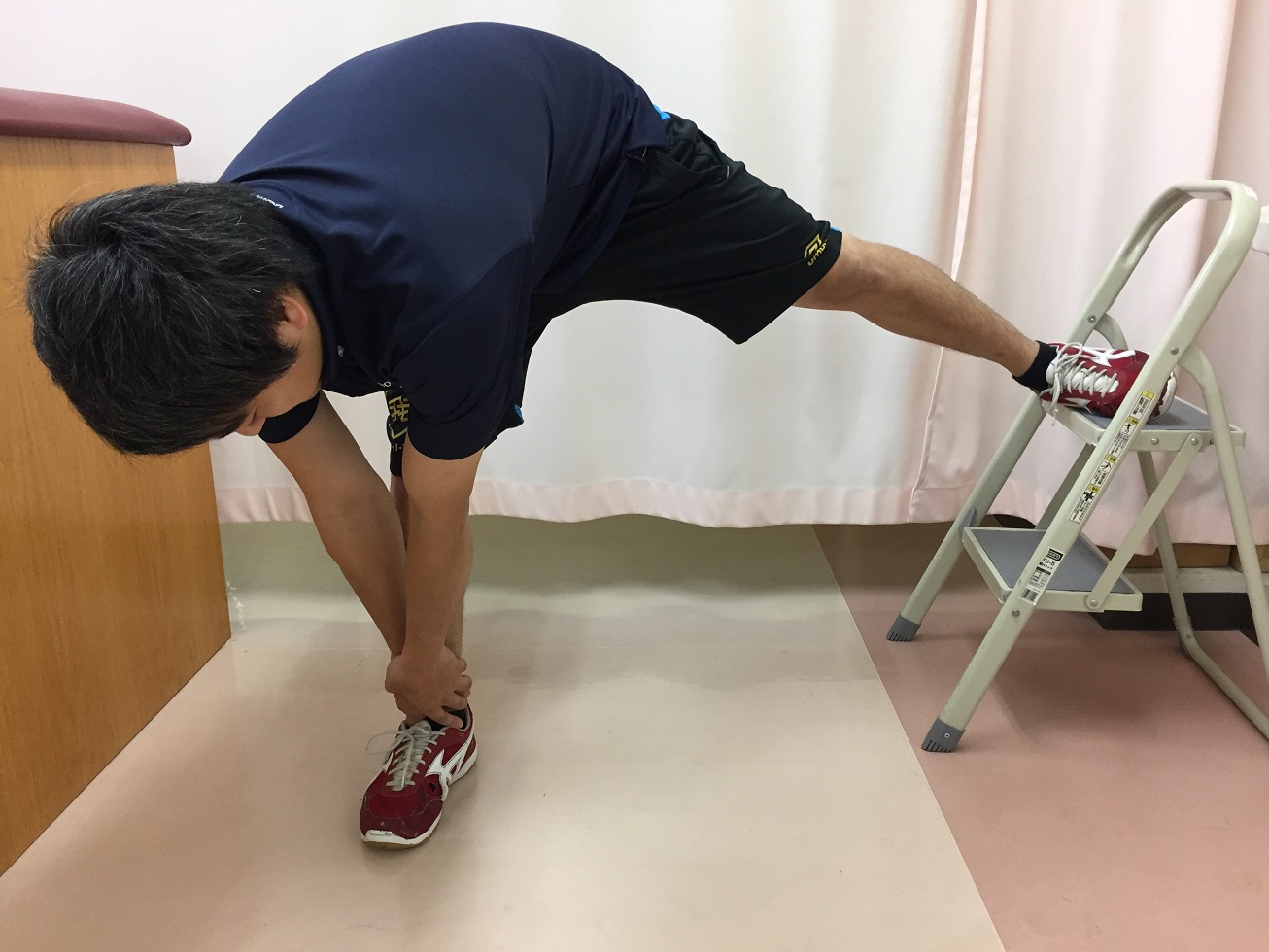
Place the leg on the step ladder and bend forward to the side of the support leg
Knee extension (sitting open leg)

With right and left

Finally, this is done in the middle. The trainer holds the legs and feet in place so that the open legs do not close.
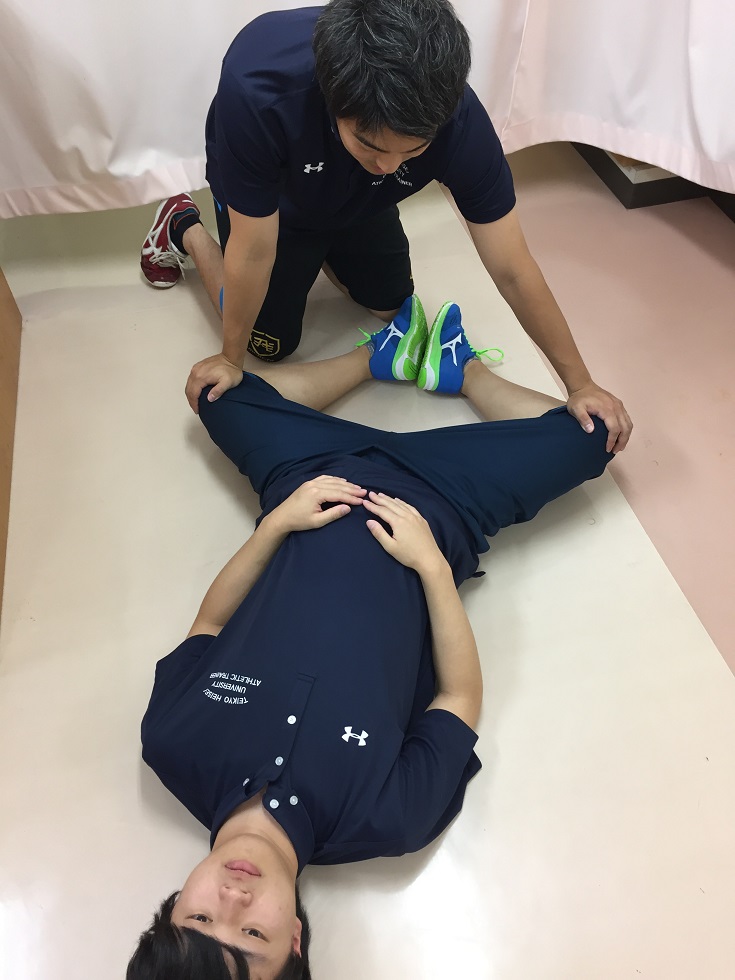
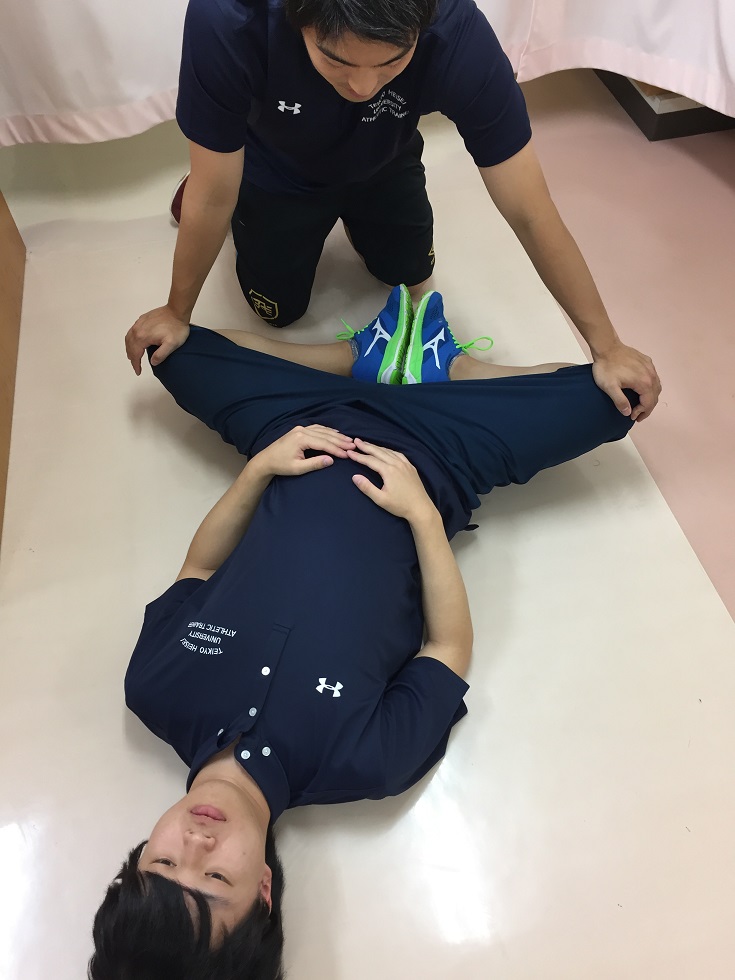
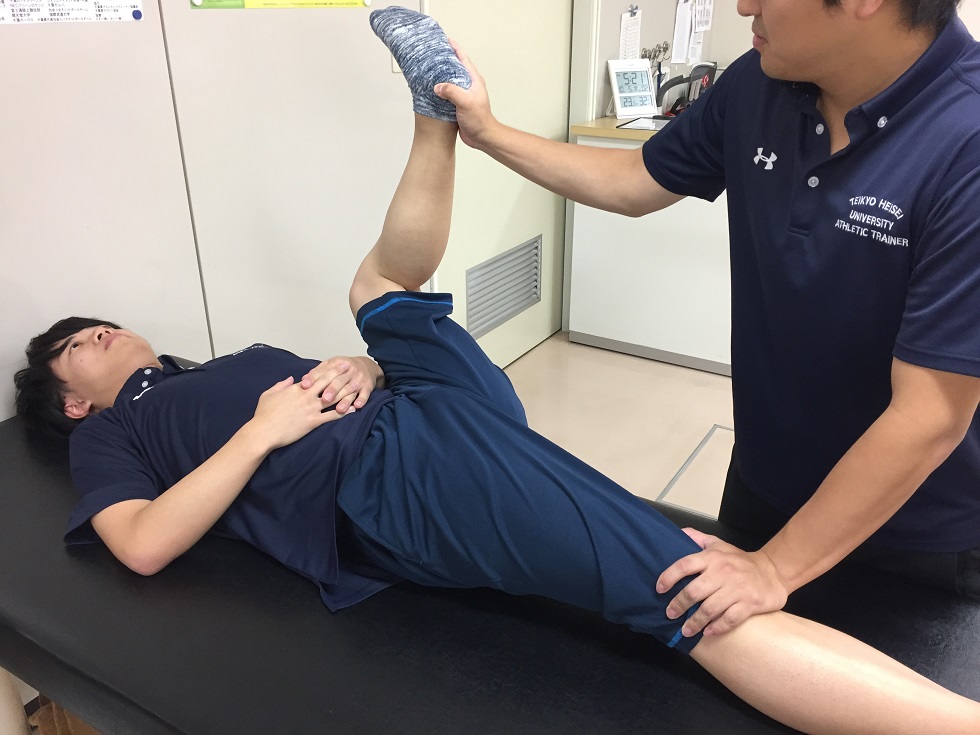
Knee extension (supine)

The trainer holds the opposite leg by pressing with the hand to prevent closure.
Knee extension (sitting position)

The trainer pushes the knee toward the floor. It is done by changing the angle of flexion of the knee joint. Stretching the knee joint with deep flexion.

Stretches with curvature of about 90 degrees. This is also more effective when the trunk is bent forward.
Knee flexion (supine)
Similarly to the sitting position, the knee joint should be angled.

Can be done unilaterally
Extensor (gluteus maximus, hamstrings)
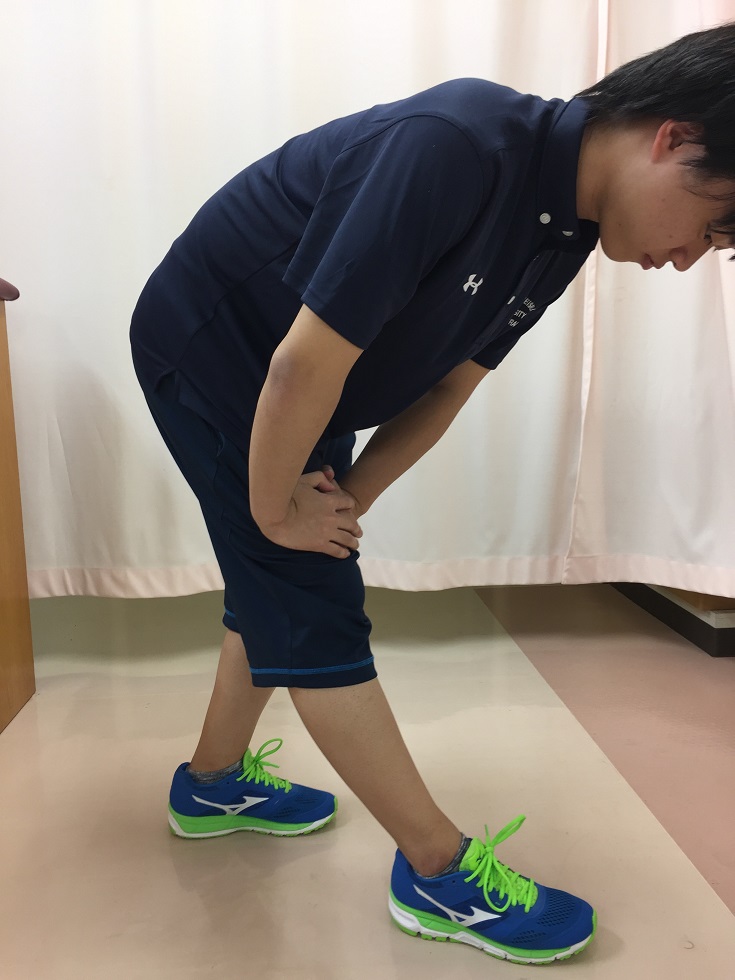
From the upright position, the stretching leg is bent forward slightly.

The legs can also be crossed.
Knee flexion
The trainer keeps the opposite leg from rising.
Knee extension

The trainer should keep the contralateral foot from rising.
Flexion to extension: first in flexion and then in extension.
