Ankle sprains


Mitsutoshi Hayashi
Mitsutoshi Hayashi
Doctor of Medicine, specialist in the Japanese Society of Rehabilitation Medicine, specialist in the Japanese Society of Orthopaedic Surgery, specialist in the Japanese Society of Rheumatology, staff to strengthen JOC, and sports physician certified by the Japan Sports Association
Ankle sprains
Disease Overview
The ankle joint is one of the most important and sensitive joints for athletes. Ankle sprains (ligament injuries) are the most common and among the more severe sports injuries, but they are often considered less serious and become chronic.
Cause and mechanism of onset
Anatomy
The ankle joint consists of three bones: the tibia, fibula, and talus; the lateral (fibular) side is surrounded by the anterior talofibular ligament, the posterior talofibular ligament, and the calcaneofibular ligament (Figure. 1). The medial (tibial) side is protected by a strong ligament called the deltoid ligament.
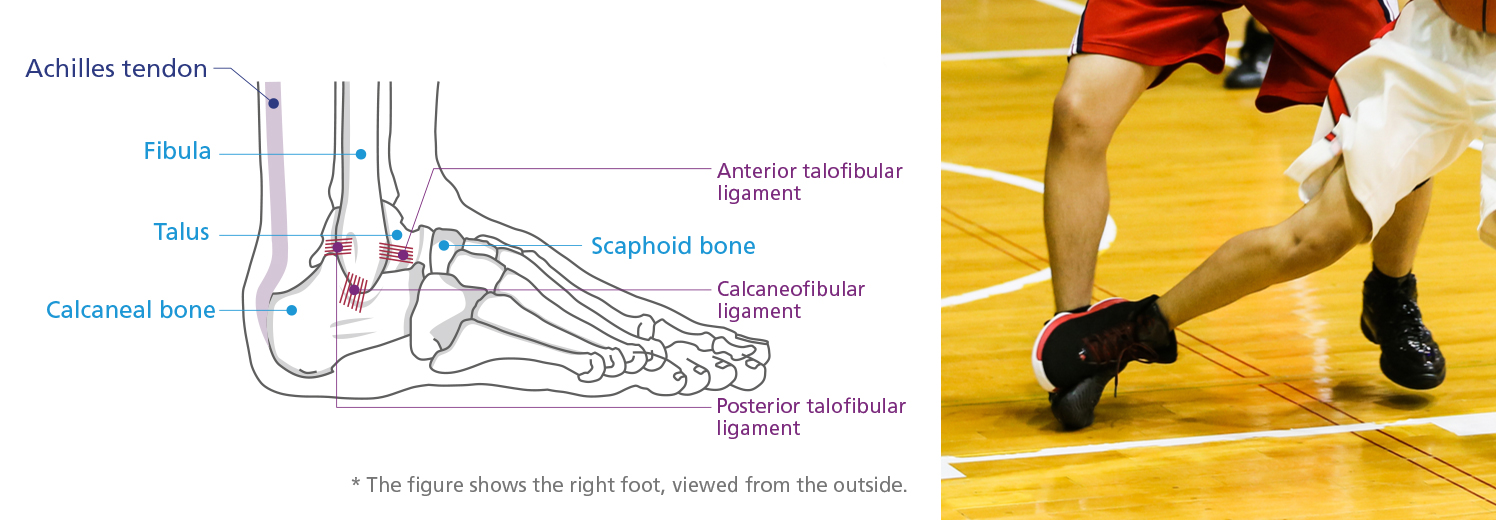
Figure 1 Ligaments of the lateral ankle joint.
Cause of the injury
The ankle joint is a joint that is more flexible in the inversion direction than in the eversion direction. Sliding or stepping on a foot can cause abrupt inversion movement and stretch or tear the outer anterior talofibular ligament. Many injuries are varus sprains, which damage the outer ligaments.
Ankle injuries are particularly common in volleyball and basketball. It is the most severe case that the inversion sprain is occurred when the athlete step on the others’ foot. (Photo 1). Sliding on the floor and twisting the feet (self-induced injury) are more likely to result in moderate injuries, most often in contact sports, such as soccer, rugby, or American football, as well as in baseball sliding, gymnastics, and tennis. Occasionally, medial side of the ankle gets injured from eversion. (Photo 2).
Injuries occur at all levels of sports, from recreational to the top-level .

Photo 1: Lateral side of the ankle which gets eversion sprain with swelling and bleeding under the skin

Photo 2: Medial side of the ankle which gets eversion sprain with sprain
Diagnosis
For inversion sprains, lateral tenderness, fluctuance due to inversion stress, and laterality are diagnosed.
X-rays can be used to check for fractures, to check for spicules, to perform a stress X-ray to check for ligament loosening (Photos 3 and 4). Lately, MRI and ultrasound examination are adopted to diagnose in detail.
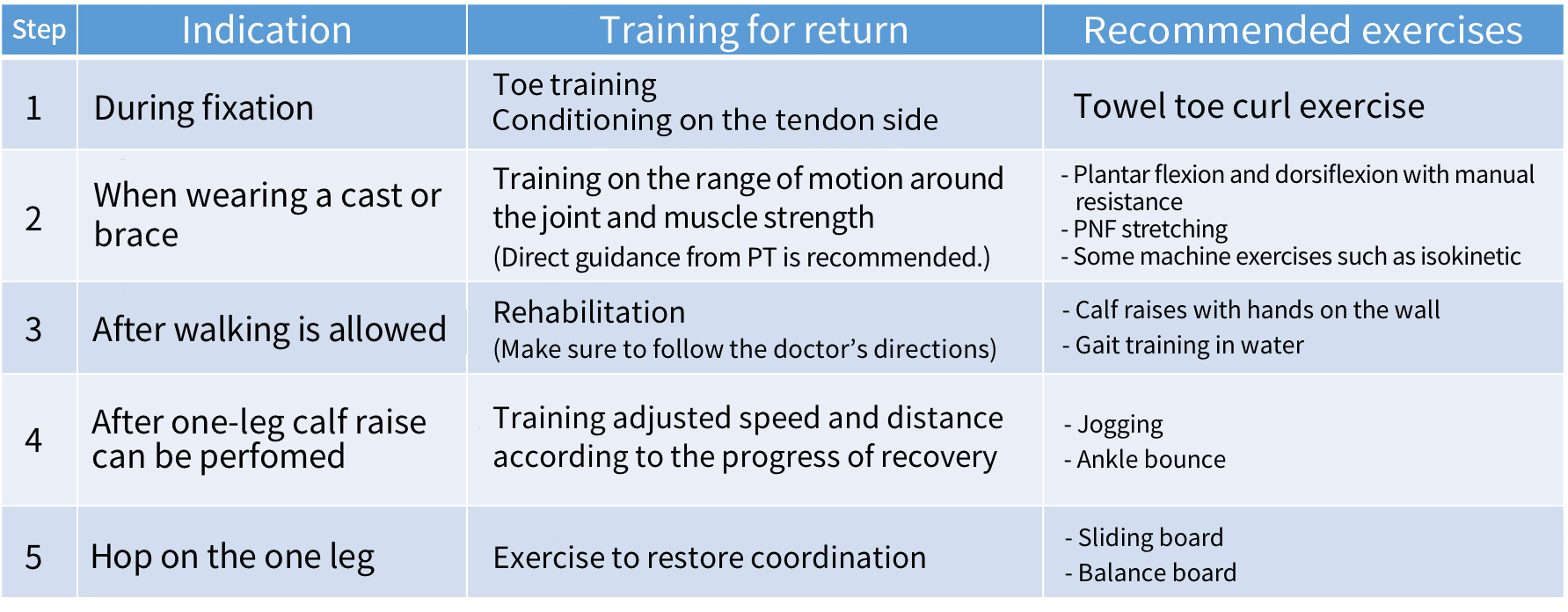
Treatment and rehabilitation
During the acute phase, after the injured area is identified, and a RICE procedure is proceeded with by splinting, bandaging, taping, and icing (Photo 5) to keep the person at rest with the limb elevated. People who have severe pain in the ankle during walking should see an orthopedic doctor, preferably a sports doctor. The three levels of injury help determine treatment and rehabilitation methods.
Achilles tendon stretching is important in the early stages of an injury because the ankle may be limited in movement (Photo 6). Taping and ankle braces have been used for solution in return to competition because they allow plantar dorsiflexion action with limitation of inversion movements. (Photo 7).
1st degree sprain: Little ligament damage and mild tenderness, which allow patients restart sports activities within 2-3 days. They can walk or run lightly.
2nd degree sprain: Partial ligament rupture, with tenderness, swelling, and inability to walk. Return to competition takes 2 to 3 weeks. Braces, taping, and splinting are needed. Please seek medical diagnosis for this case.
3rd degree sprain: Complete ligament tears cause tenderness, swelling, warmth, and bleeding under the skin, making walking difficult. It takes 1 to 2 months to return to competition. Treatment at the hospitals (rigid immobilization with a cast or brace or suturing of the ruptured ligaments) is needed.
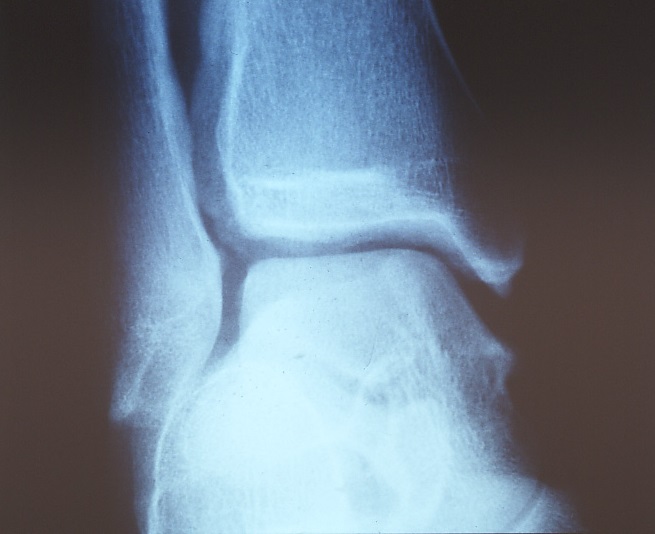
Photo 3: The ankle is preserved at a glance
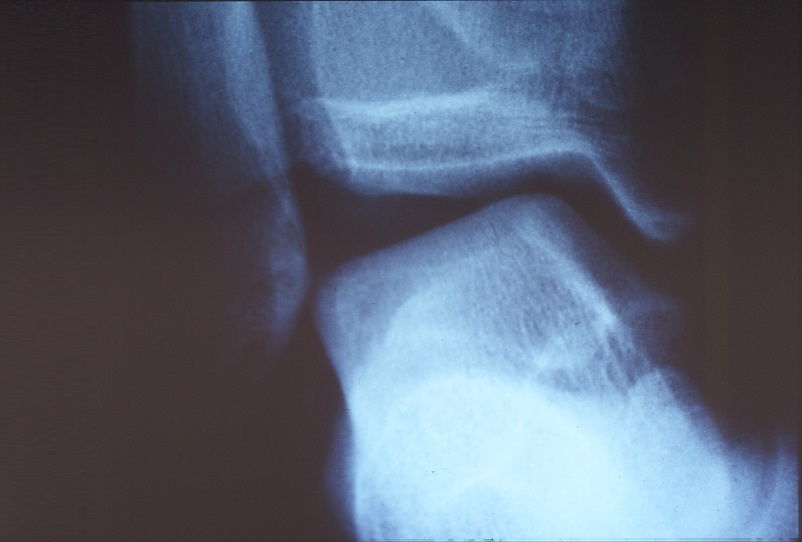
Photo 4: The same ankle in the stress
Precaution
When the athlete gets first ankle sprains, adequate immobilization and enough terms of rest are required because joint mobility persists and causes repeated chronic sprains. Aggravation may also cause impingement syndrome and cartilage degeneration of the ankle joint.

Photo 5: Ankle icing
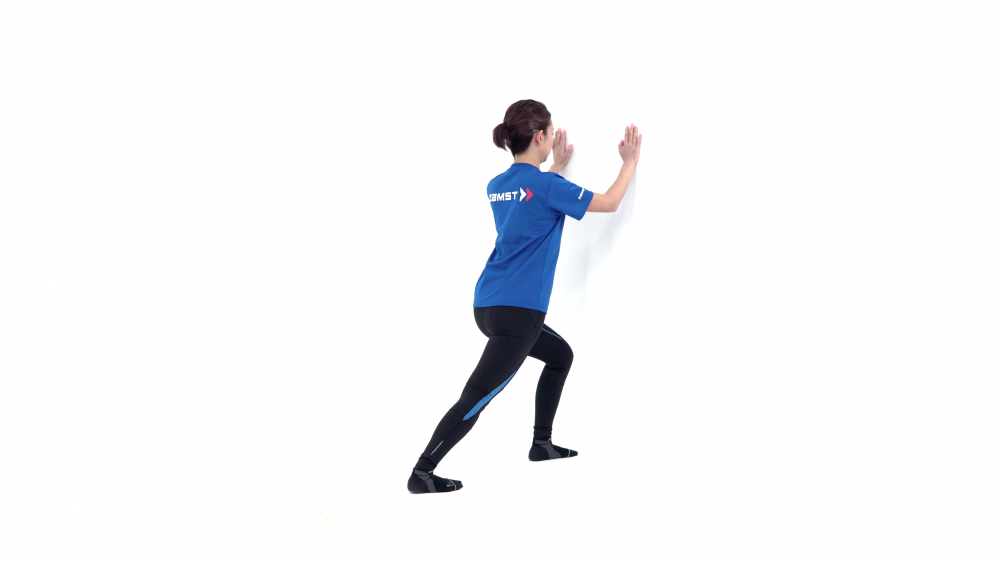
Photo 6: Wall press. Please be aware that the calf and Achilles tendon are extended and ankle is dorsiflexed. A good example is the posture in the rugby.

Photo 7: With ankle braces
Key Notes
It is important to train the ankle joint toward four directions, anterior, posterior, lateral and medial directions. Especially, strengthening the fibular tendons instead of the damaged lateral ligaments (motion in the ankle eversion direction) for return to competition.

Yoshizumi Iwasaki
Yoshizumi Iwasaki
NATA certified athletic trainers, certified athletic trainers from the Japan Physical Education Association, and chairman of the Japan Core Conditioning Association (JCCA)
Ankle sprain (trainer stitch)
Prevention
Please use supports , tapes, etc. When you taping up, please refer to the specialized books, etc. according to your needs.
There are different types of supports in the market (Medical Edition Photo 5). They are different in terms of functions as the ankle supports. It is recommended that you try them on when you choose as like shoes fitting.
On-site evaluation and first aid
Ankle sprains (ligament injuries) are injuries caused by “twisting” the ankle. First, the severity of the injury can be determined to some extent by the circumstances in which it occured.
(1) The patient cannot move
(2) The patient reports immediately leaving the practice (game) on his or her own.
(3) The patient reports after completion of play.
(4) The patient reports after completion of practice (game).
(5) The patient reports the following day and later.
Because the intensity and sensation of pain vary considerably among athletes, reporting the next day or later should not dictate as a minor injury. However, it is necessary to assume a severe injury when the victim is transported on a stretcher without being able to move himself or herself.
HOPS
When an injury occurs in a sport scene, the trainer listens carefully (H: history) to determine the circumstances, then looks at the affected area thoroughly (O: observation), touches the parts(P: palpation), and checks for movement (S: special test).
History: Hearing: Ask the person to explain what happened. Patients with any significant indicators at that stage, such as “broken” or “the sound, ” should be transferred to the hospital.
Observation: Check the injured parts.
Palpate: Check for fever and swelling. If there are any obvious abnormalities, please take them to the hospital.
Inspection: Look at the affected area. People who have obvious deformities, swelling, or discoloration should go to the hospital.
Special test: Even if you can check the three steps above, there are cases in which the person can’t stand up, can’t walk, or can’t run. A doctor should be consulted to determine if the patient can actually move and if he or her has a functional abnormality.
Once all HOPS checks have been taken, take precautions such as taping and perform retest (Table 1). Basically, consider the inversion sprain of the ankle should be examined by doctors.
As with other sports injuries, the basis of first aid is RICE methods for ankle sprains. The injured part is rested with immobilization (R=Rest) and the injured part is cooled with ice (I: cooling = Ice). The injured part is then compressed (C: Compression) and raised above the heart (E=Elevation). When icing, using ice that is too cold or ice packs using chemical reactions may cause frostbite. However, fresh ice produced by an ice-making machine can be applied directly to the affected area.
Caution! Compartment syndrome* is a risk when the pain is so severe that the temperature is increased and the numbness spreads, and the person wants to scrape off the affected area during icing. Raise the limb to the level of the heart and promptly go to the hospital. Emergency surgery may be needed.
* A circulatory (blood flow) disorder caused by increased pressure within a compartment surrounded by fascia, interfascial septum, bone, or periosteum. If pressure is not lowered, muscle necrosis and sequelae occur.
Reconditioning
If surgery is indicated for a third-degree injury, rehabilitation may be performed in the hospital under the guidance of a physical therapist. The main objectives are to restore range of motion and muscle function. Even if the person does not go to the hospital, the person should be reconditioned after rest to obtain flexibility, strength, and balance (including joint stability). As you can see in the Medical Edition, stretching should be done firmly, particularly the flexibility of the Achilles tendon, which is closely related to the ankle sprain.